Microtia
the center of MicrotiaWhat is microtia
What is microtia?
Microtia is known to occur in 1 out of 5,000-7,000 newborns (statistics vary slightly by race and country), and it is a deformity caused by an abnormality in Hillock
development that forms ears in the fetus.
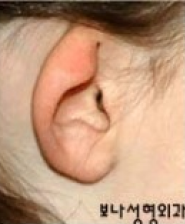
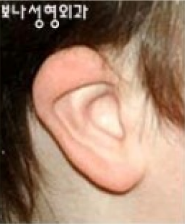
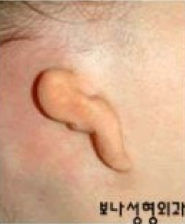
Microtia can be divided into five types according to the shape of the remaining ear:
1) lobular type, 2) small concha type,
3) concha type, 4) Microtia associated with low hair line, 5) anotia.
The typical microtia (ear lobe type) without an earhole is the most common.
-

lobular type
-

small concha type
-

concha type
-

Microtia associated with low hair line
-

anotia
In other cases, the Marx classification method is also used.
-
 Grade Ⅰ
Grade ⅠThe ear is small, but most of the shape of
the normal ear remains, and the ear canal
is usually present. -
 Grade Ⅱ
Grade ⅡThe ear is also small, but part of the shape of the
ear is missing, and the ear canal may or may not be present.
When there is no ear canal, it is called aural atresia. -
 Grade Ⅲ
Grade ⅢOnly a part of the ear lobe remains, and
the location is different, and most of
them have no ear canal. -
 Grade Ⅳ
Grade ⅣA state in which there is almost no shape
of the ear (anotia)
Microtia and hearing
In most cases of microtia, the ear canal and the middle ear are often absent or underdeveloped because they originate from the same tissue at the developmental stage. However, having no ear canal does not mean that there is no hearing at all, and the person can hear vibration through bone conduction, so hearing is about half that of normal ears. Fortunately, about 90% of patients with microtia have microtia on only one side, not requiring hearing aids, and there is no problem in hearing or speaking if the normal ear is healthy.
Causes of microtia
The exact cause of microtia is unknown. If their child has microtia, parents ask whether it is hereditary, but when parents and siblings have microtia, the probability that the child will have microtia is only about 1-2%.
Accompanied malformation
Most people with microtia have no problems other than their ears. However, the facial part on the microtia side may be less developed in about 1/3 patients, although there are some differences. (Hemifacial microsomia) If not severe, correction is not necessary, but if severe, correction is necessary.
Correction period
The correction period may vary depending on the surgical method, but making an ear using one's own chest cartilage is the most common and widely used method. The upper grades of elementary school, when the chest cartilage grows to a certain extent and the chest deformity does not occur easily even if a large amount of chest cartilage is removed are the right time for correction. Since the method of reconstructing the ear with artificial materials does not use chest cartilage, reconstruction is possible even at the age of 5-6 years, which is earlier than the method of reconstruction with chest cartilage.

Correction methods
Correction methods can be mainly divided into a method using one's own chest cartilage and a method using artificial materials. The most common method is to use chest cartilage, and even after surgery, the ears made will also grow as the child grows. On the other hand, methods of using artificial materials include a method of inserting a porous material called Medpor and covering it with autologous tissue as a method that began in the United States in the 1990s and was developed. This method has the advantages that early surgery can be possible at 5-6 years of old because the autologous cartilage is not used. Because the autologous cartilage is not used and there is no chest tissue in the chest, but it has the disadvantages that there is a possibility of exposure or inflammation because artificial materials are used. With more than 30 years of experience, however, most of these disadvantages have been rectified.
Activities after microtia reconstruction
Basically, there are no activity restrictions of reconstruction using autologous cartilage. If the wound is completely healed after reconstruction, you can exercise or swim after about 5 weeks. No special device is required to protect the reconstructed ear.
Consult with Bona Clinic.
information
-
Weekdays
10:00 ~ 19:00 Lunch time 13:00 ~ 14:00 -
Saturday
10:00 ~ 16:00 Lunch time 13:00 ~ 14:00 -
Directions
Line 3 Apgujeong
Station Exit 4 150m straight
(Line 3 Apgujeong Station Exit 4, 150m straight) Business registration. 211-09-47985
Copyright © 2023 Bona Clinic All RIGHTS RESERVED.